Spinal Tumour
|
The spine, also called the backbone, is a flexible column of linked bones (vertebrae), muscles, tendons, and other tissues that extend from the base of the skull to the tailbone. It includes three protective membranes that encase the spinal cord and the fluid surrounding it. The spine provides structural support for the body and facilitates movements such as twisting and bending. The column of nerves in the spinal cord transmits signals to the brain to control movement, sensation, and bladder and bowel function. Tumors can develop in the vertebrae, nerves, and other tissue throughout your spine. Some spine tumors, such as astrocytomas, occur more commonly in children and adolescents Fewer than 10 percent of spine tumors begin in the spine. These tumors, called primary tumors, may be benign or low-grade, malignant growths that are slow growing, or high-grade tumors that grow very aggressively. The vast majority of spine tumors are metastatic. These tumors arise from cancer that begins in another part of the body, such as the lungs, breasts, colon, prostate, kidneys, or thyroid gland. Sarcomas – cancers of the bone, muscle, or connective tissue – can also spread to the spine. |
 |
Types of Spine Tumors
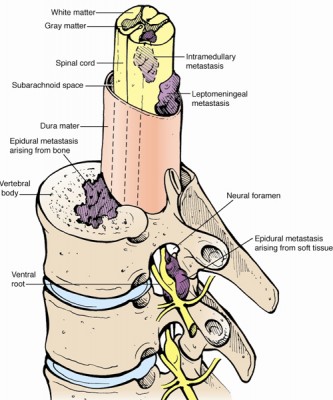 |
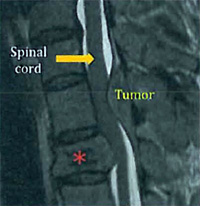
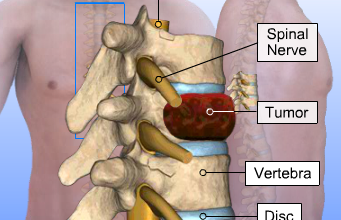
Spinal MetastasesMost primary and metastatic spine tumors are epidural tumors. These tumors grow in the bones of the spine. As they grow, they can compress the spinal dura – a thick sac that contains the spinal cord, nerve roots, and spinal fluid.
Nerve plexus tumors such as neurofibromas and ganglioneuromas occur next to the spine in the nerve plexus, a network of intersecting nerves that transmits signals from the brain to the arms or legs. |
Symptoms
As a spine tumor grows, it can replace bones or compress nerves, resulting in compression fractures or reduced blood supply to the spinal cord. Often, the first symptom of a spine tumor is the pain caused by these changes. The time of day at which the pain occurs can provide important information about the tumor.
Pain that occurs mainly when you are moving – mechanical pain – usually means that the tumor is causing weakness or instability in the bones of the spine.
Pain experienced primarily at night or in the early morning that lessens with movement is often an early sign that the tumor has spread. This is because your adrenal gland, which makes steroids during the day to help prevent inflammation, becomes less active when you are sleeping.
Spine tumors that are close to major nerves can disrupt the nerves’ ability to receive and send messages between the body and the brain. This can cause neurologic symptoms such as:
- weakness, tingling, or numbness in both legs or arms
- difficulty walking or balancing
- sensory problems
- loss of bowel and bladder control
Tumors within the spinal cord generally cause detectable symptoms, while spinal tumors outside of the cord may develop for some time before symptoms emerge. Common symptoms include:
- Back pain
- Cold sensation in the legs, feet or hands
- Loss of bowel control
- Loss of sensation, particularly in the legs
- Muscle weakness and difficulty walking
- Muscle contractions or spasms
The first test to diagnose brain and spinal column tumors is a neurological examination. Special imaging techniques such as computerized tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) are also performed.
Laboratory tests include the electroencephalogram (EEG) and the spinal tap. A biopsy, a surgical procedure in which a sample of tissue is taken from a suspected tumor, helps doctors diagnose the type of tumor.
Treatment
- Surgery
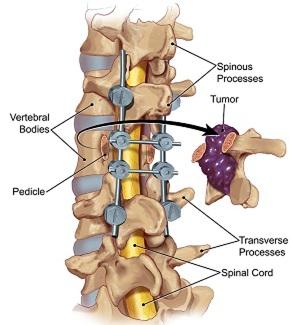
While surgery is increasingly recommended for benign and malignant primary spinal cord tumors, the role of surgery in spinal metastasis, or cancer that has spread to the spine, is controversial. Recent developments in imaging as well as new surgical tools and techniques, such as ultrasonic aspirators and lasers, have significantly expanded the role of surgery as an intervention.
For metastatic tumors with spinal cord compression, some neurosurgeons may perform surgery in selected patients to relieve pressure and pain, reconstruct or stabilize the spine, preserve mobility and bowel and bladder function, and to maximize quality of life. Some doctors may only recommend surgery for patients with a single metastatic tumor and no evidence of cancer growing at another site.
- Radiation Therapy
Most patients with primary spinal cord tumors will not require radiation therapy. Radiation, however, is used to treat spinal cord compression due to metastatic cancer or cancer that has spread from other locations. Other targets of radiation include some primary cancers of the spine and more rarely, benign or low-grade spinal cord tumors that cannot be completely removed surgically.
The spinal cord is even more sensitive to the effects of radiation than the brain. Our radiation oncologists work carefully to minimize the risk of radiation-induced damage to normal spinal tissue since it can be progressive and irreversible. The thoracic spinal cord segments, or those located near the chest where half of all spinal tumors occur, are the most sensitive to the effects of radiation.
Radiosurgery with an advanced device called the CyberKnife may be an option for some patients. The CyberKnife is a painless, non-invasive threatment that delivers high doses of precisely targeted radiation to destroy tumors or lesions. Radiosurgery minimizes radiation exposure to healthy tissue surrounding the tumor.
The CyberKnife uses a robotic arm to deliver highly focused beams of radiation. The flexibility of the robotic arm makes it possible to treat areas of the body, such as the spine and spinal cord, that cannot be treated by other radiosurgery techniques.
- Chemotherapy
Chemotherapy, similar to that used for brain tumors, may be recommended in adults for spinal gliomas that progress after surgery and radiation.
Chemotherapy is the use of drugs to kill cancer cells. Your doctor may use just one drug or a combination, usually giving the drugs by mouth or by injection into a blood vessel or muscle. Intrathecal chemotherapy involves injecting the drugs into the cerebrospinal fluid.
Chemotherapy is usually given in cycles: a treatment period followed by a recovery period, then another treatment period, and so on. Patients often do not need to stay in the hospital for treatment. Most drugs can be given in the doctor's office or the outpatient clinic. However, depending on the drugs used, the way they are given and the patient's general health, a short hospital stay may be necessary.
Getting an accurate diagnosis for a spinal tumor is very important. It helps your doctor plan your care and may help increase the chance of successful treatment.
If you have symptoms that may signal a spinal tumor, your doctor (Neurosugeon) will examine you and ask you questions about your health, your lifestyle and your family medical history.